If you lead nursing, clinical, or quality operations at a Joint Commission-accredited organization, you’ve probably already heard that The Joint Commission and the National Quality Forum (NQF) are aligning their patient safety reporting frameworks as of January 2027. The intent is to have a unified standard that reduces your reporting burden.
This consolidation is grabbing the headlines in healthcare news, but there’s more to the story for clinical leaders. This alignment signals changes to accountability and puts more emphasis on preventable events.
Falls and pressure injuries have been a focus of patient safety reporting for over two decades. Starting in 2027, consistent definitions for both events will close gaps created by state-by-state interpretations and make performance data easier to compare across all accredited organizations.
This raises the bar for demonstrating management of these risks. Here’s what the change means for your setting, and where you should focus to prepare.
What the 2027 Transition Actually Changes and What It Doesn’t
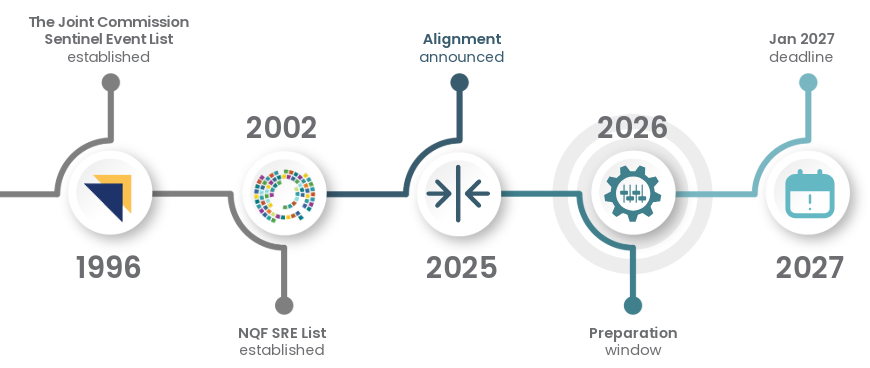
Here’s some quick context around what led to the 2027 changes.
The Joint Commission’s SE List qualified events based on outcome (death or serious harm), while the NQF’s SRE List required both severity and preventability, and the two differed further in naming conventions and structure.
Starting January 2027, The Joint Commission will adopt the updated NQF SRE List as the foundation of its Sentinel Events List, retaining three legacy workforce safety events from the original SE List.
What doesn’t change: Reporting to the Joint Commission remains voluntary. Also, the internal response obligations already in place for accredited organizations, including identifying sentinel events, conducting a root cause analysis, and developing a corrective action plan, remain in place regardless of whether an organization reports externally.
What does change: The events that trigger those internal obligations. The 2027 transition brings consistent definitions and categories to more than 23,000 accredited organizations in the U.S.
This standardization matters for health systems managing accreditation across multiple facilities. The same definitions and thresholds will apply everywhere, making cross-facility benchmarking more meaningful and regulatory scrutiny more consistent.
Why Falls and Pressure Injuries Are at the Center of the New Framework
Of the 28 SREs on the updated list, two are especially relevant to how clinical teams monitor and respond to patient status on an ongoing basis.
Falls resulting in serious patient harm have been on the SRE list for over 20 years. The updated framework retains them, and the unified standard means organizations will now be measured against a common definition, making it easier to identify where gaps exist and where improvement is needed.
Under the new framework, the obligation isn’t new. But the consistency and expectations are. Organizations will need to demonstrate that their prevention protocols correspond with their patient population’s risk.
Pressure injuries are more precisely defined under the unified standard. The scope narrows to Stage 3, Stage 4, unstageable, and deep tissue injuries acquired after admission that are likely avoidable and require major intervention. Events that reflect a care failure will be distinguishable from those tied to unavoidable clinical circumstances.
What the Deadline Means for Hospitals vs. Skilled Nursing Facilities
Preparing for the deadline is different for hospitals and health systems than for skilled nursing (SNF) facilities.
Hospitals and Health Systems
This is where the alignment has the sharpest near-term impact. Join Commission-accredited hospitals are the primary audience for the new unified standard, and 2026 is explicitly intended to be a preparation window.
The Joint Commission and NQF have published transition guidance and crosswalk documentation, and hosted webinars to help with updating reporting and quality frameworks before the deadline.
For clinical operations leaders, the practical question is: do your current monitoring and documentation practices give you clear visibility into fall risk and pressure injury risk at the patient level in real time?
Many hospitals can easily answer yes for patients on high-acuity units. That’s where monitoring resources are concentrated. For general medical and post-surgery floors and anywhere clinical bandwidth is stretched, saying yes gets harder. Those are also the settings where falls and pressure injuries are most likely to go undetected until harm has occurred.
The expectation with the unified framework is that organizations have systems and protocols in place to demonstrate proactive risk identification, not just reactive response.
Skilled Nursing Facilities
For SNFs, falls and pressure injuries are already deeply embedded in daily operations, tracked through CMS requirements, Minimum Data Set (MDS) reporting, and star-rating metrics. That existing infrastructure means the January 2027 announcement carries less immediate disruption than it does for hospital teams. The difference is subtler and more impactful over time as terms get standardized and cross-institutional benchmarking occurs.
The modifications and variabilities that made state-by-state comparisons difficult are being reduced. For SNF administrators and directors of nursing, there’s less immediate pressure around the deadline, but increasing pressure from the combination of family expectations, CMS oversight, and star-rating implications.
The question worth asking here isn’t whether you’re meeting the current reporting requirements. It’s whether your prevention protocols and internal response processes can hold up under a more consistent national standard.
![]()
The Visibility Gap Hindering Fall and Pressure Injury Prevention
Preventing falls and pressure injuries comes down to the same basic need: changes in patient status need to be identified earlier so interventions can happen sooner. How can clinical teams get ahead of these events?
Unusual restlessness, changes in activity levels, prolonged stillness, and changes in movement frequently precede a deterioration event. Yet staff can’t be in every room with every patient all the time. Patients who need attention don’t always call for it, and early signals are easy to miss when staff are overextended and running at capacity.
Scheduled rounds, shift changes, and overnight hours limit how much time staff can spend with any one patient. Manually documenting repositioning can introduce inconsistencies. The volume of call lights and bed alarms can make it difficult to identify urgent from routine.
The result is a visibility gap, where patient status is effectively unknown until something goes wrong.
Preparing for the 2027 transition requires a critical eye to identify gaps in your organization and decide how you will close them.
The goal should be to give your clinical teams the tools, information, and protocol they need to prioritize their attention and act early. Unless intervention happens before a patient falls or before a pressure injury progresses, an avoidable event becomes a sentinel event.
How to Prepare for the Joint Commission’s Sentinel Event Changes
For organizations beginning their 2027 transition planning, a few practical areas should be prioritized now.